


Early Detection for Cancer Is a Risky Business
 Accepting an examination of your body parts in an effort to find cancer earlier means you are willing to risk your life today for the theoretical possibility that you will gain extra years in the distant future.
Accepting an examination of your body parts in an effort to find cancer earlier means you are willing to risk your life today for the theoretical possibility that you will gain extra years in the distant future.
For example, I have known perfectly healthy people in their forties suffer a perforation of their bowel during a routine colonoscopy and die—all from an effort to prevent colon cancer in their sixties or seventies.
While attempting to prevent one death from colon cancer with 1,000 examinations, two people may suffer from this potentially fatal complication (in addition to other complications, such as those from bleeding and anesthesia). Fortunately, similar cancer benefits can be had with a safer sigmoidoscopy examination, at almost no risk, or a test of the stool for blood or DNA at no risk of physical harm.
Screening for cancer is “disease mongering” at its worst. By casting a large net with early detection schemes, people are roped into laboratory tests, imaging, doctors’ office visits, biopsies, surgeries, radiation treatments, pharmaceuticals, chemotherapies, and hospitalizations. Disease mongering turns people into patients, and few will benefit.
Potential patients must become fully informed about the risks and benefits of breast, vaginal, prostrate, and colon examinations before stepping onto the “screening” highway, which more often leads to death and disability than a prolonged life. Recommendations call for shared decision-making between doctor and patient. However, this approach is unrealistic because patients do not have the fundamental medical knowledge necessary to understand complex health issues. Even more concerning (as you will learn below), primary care doctors fail to understand the risks and benefits of the very screening tests that they are recommending to hundreds of millions of their customers.
If more harm than good results from screening and early detection methods are avoided, then how should tumors, like breast cancers, be found? By casual examinations such as when bathing or showering. If a lump is found, then this abnormality should be brought to the attention of the medical doctor. (In almost all cases I recommend simple removal of the obvious tumor, only.) In contrast, self or clinical breast exams can create high anxiety, whether or not any problems are found, and in most cases lead to many unnecessary and costly tests, biopsies, and surgeries with no gain in quality or quantity of life.
Early Detection Is Really Late
“Early detection” is a misnomer. At the time of diagnosis, a solid tumor developing in the breast, colon, lung, or prostate has grown to one centimeter (1/2 inch) in size and contains 1 billion cells. The average time for this growth to reach a detectable size is 10 years. Cancer destined to spread to other vital organs has already done so. Fortunately, most tumors found during screening are destined to be non-troublesome and are likely to continue on their non-lethal (benign) course.
By understanding the natural growth history of cancer you will understand why early detection methods fail and why, after discovery, treatment should be conservative. For example, I recommend a simple lumpectomy for breast cancer (instead of removing the entire breast or a lumpectomy with radiation) and simply “burning off” cancers of the lower bowel (instead of removing entire sections of bowel).
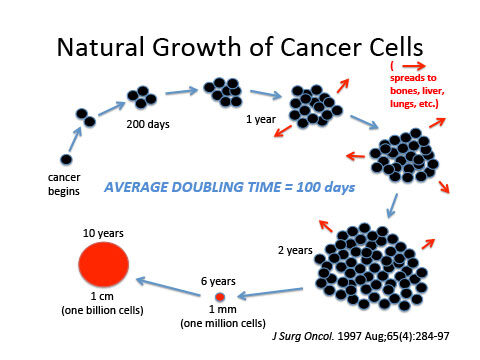 |
Cancer begins as one misguided cell dividing at its own free will, irrespective of its neighbors’ welfare. The average doubling time is every 100 days (3½ months). Approximately 30 doublings must occur for a cancer to reach a detectable size. Basic math proves this to be, “late detection.” Cancer cells spread early in the disease via the venous system to vital organs (where many metastatic cells will divide at a similar rate to the original tumor cells).
Researchers have understood the natural growing history of solid cancers, like those found in the breasts, colon, lung, and prostate, for more than a half-century. Consider this 1977 statement delivered at the, “Conference on Breast Cancer: A Report to the Profession” sponsored by the White House, the National Cancer Institute, and the American Cancer Society: “If the time required for a tumor to double its diameter during a known period of time is taken as a measure of growth rate, one can calculate by extrapolation that two-thirds of the duration of a breast cancer remains undetectable by the patient or physician. Long before a breast carcinoma can be detected by present technology, metastatic spread may occur and does in most cases.”
Misunderstanding Perpetuates Malpractice
Unfortunately, most people, and even their primary care physicians, mistakenly interpret “improved survival” and “increased detection of cancers” as evidence that screening saves lives. Few correctly recognize that only reduced mortality (a longer life) in a randomized trial constitutes evidence of the benefit of screening.
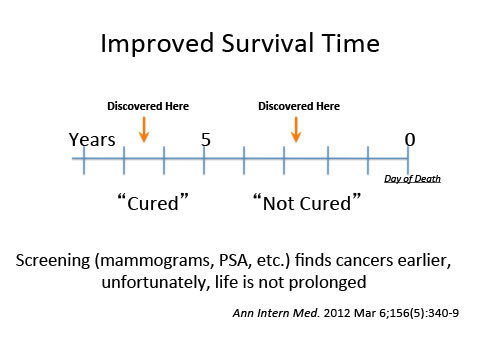 |
The first fatal error is in believing that “improved survival” is beneficial. The length of survival is measured from the time of diagnosis until death. By finding disease earlier with screening programs the diagnosis is made earlier, but the day of death remains the same. The patient does not live longer (no improvement in mortality), but he or she is made aware of his or her illness for more years by finding it earlier. Without argument this awareness leads to enhanced profits for many medical industries.
False hope is created by early detection. Cancer patients have been told, “If you live five (5) years or longer after diagnosis, then you are cured.” Based on this definition, cure by early detection is experienced by as many as 90% of breast cancer patients. (Yet, to repeat, they live no longer.)
The second error in thinking arises from the belief that finding more cancers benefits patients. Most cancers found by screening are over-diagnosed: they are non-troublesome and are non-lethal, and would have been of no importance if never discovered.
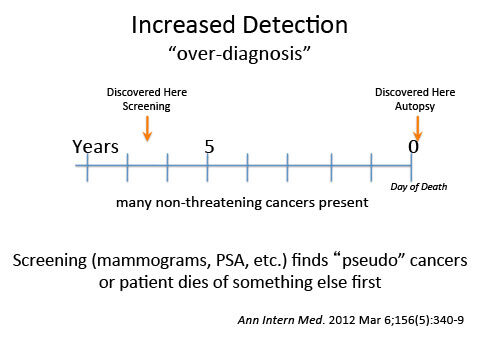 |
Cancers discovered only after death, say at an autopsy, obviously never threatened the patient’s life. The person has died of something else first, say, heart disease or old age, long before the cancer surfaced. Early detection tests uncover “pseudo” and dormant cancers. For every one person whose life is “saved by early detection,” 10 to 50 people are over-diagnosed with cancer. Meddling physicians have turned healthy people into casualties of cancer.
Looking for a Longer Life?
The true test for an effective method of screening for cancer is to improve mortality for the group undergoing the exams, compared to a control group subjected to less vigorous detection methods. By this standard, benefits from screening programs are hard to find.
 |
My belief is that the best effort for prolonging a person’s useful years is to stop the causes of their deadly diseases. Cancer of the breast, colon and prostate are examples of illnesses caused by food poisoning from consuming animal-derived foods and vegetable oils. The remedy is serious, intensive, dietary changes.
On August 29, 2014 the USPSTF made their official recommendation that doctors focus their attention on diet: “The USPSTF recommends offering or referring adults who are overweight or obese and have additional CVD [cardiovascular disease] risk factors to intensive behavioral counseling interventions to promote a healthful diet and physical activity for CVD prevention. (B recommendation).” The Patient Protection and Affordable Care Act (Obamacare) is aimed at expanding access to health care and lowering cost barriers to seeking and receiving care, particularly for high-value preventive care. Current legislation requires that Medicare and all qualified commercial health plans cover routine preventive services graded A and B by the U.S. Preventive Services Task Force (USPSTF) at no cost to the consumer.
Cancers of the breast, colon, and prostate are caused by the rich Western diet. People wanting to prevent, and those currently with, these diseases deserve the same intensive behavioral counseling interventions as do overweight patients with CVD. By applying all of the current USPSTF recommendations, the future of medical care could become focused on changing the American diet and improving health and longevity, rather than searching for more disease. (See the “free McDougall Program” for my dietary advice.)
Books and DVDs
Previous Newsletters
Discuss this newsletter with others
Recommended Articles

Three Essential Keys To a Healthy Diet

Making the Change to a Healthy Lifestyle Work, Part 3 - Cooking Techniques
Join the Conversation!
Have a question, a helpful tip, or a story from your journey? Add it below - your voice matters.