


Cleaning Out Your Arteries
This article originally appeared in the June 2003 McDougall Newsletter and has been updated in January 2023.
By John McDougall, MD
The leading cause of death in Western countries is heart disease. Possibly as many as 200,000 to 300,000 people in the United States have heart attacks every year – 1 million patients visit the hospital each year for the same reason. The third leading cause of death is another disease of the arteries, strokes. Many other diseases, from hearing loss to impotence, are also caused by closure of the blood supply to vital tissues.
The closure of arteries in various parts of the body causes all kinds of common diseases. (The disease is named for the tissue that is compromised):
- Macular degeneration (eye – loss of vision)
- Hearing loss (ears)
- Stroke (brain)
- Heart attacks (heart)
- Aneurysms (usually the large aorta in the abdomen)
- Kidney failure
- Bowel infarction*
- Degenerative disks (back pain and ruptured discs)
- Claudication (pain in legs with walking)
- Gangrene (death of tissues – like foot or leg)
- Impotence (sexual dysfunction – limp penis)
- Other kinds of infarctions*
*Infarction means sudden insufficiency of blood supply that produces an area of tissue death.
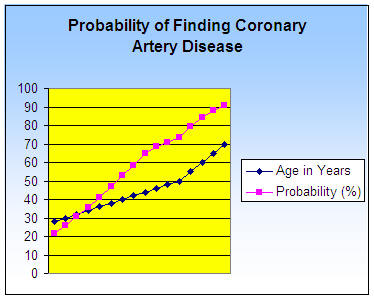
The older you are the greater your chance of artery disease.
We all start out with baby clean arteries, but that soon changes with consumption of the rich Western diet. Children raised on cow’s milk, meat, and other delicacies soon show fatty streaks (the earliest stage of atherosclerosis) – in their aorta. This damage is seen as early as 9 months of age, and all children on this diet show artery damage by age 3 years.1 These streaks eventually evolve into the plaques that are commonly seen on angiograms and at autopsy in adults.
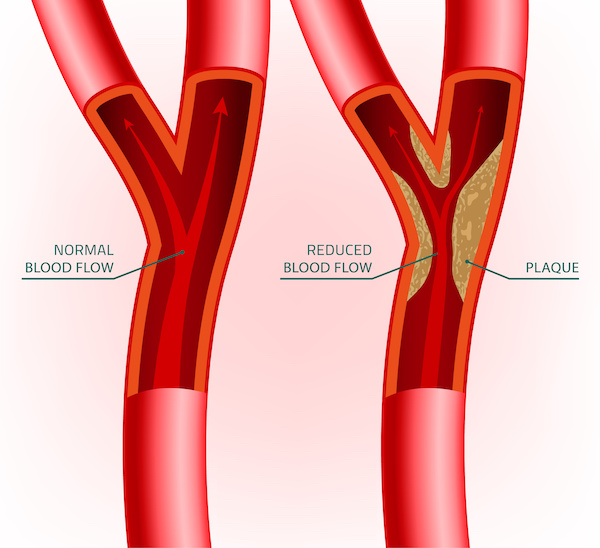
Young and Mature Blockages
Atherosclerosis is the name used for the disease that damages the arteries. The actual lesions are called plaques. Although some problems develop slowly from gradual closure of an artery due to enlarging plaques from atherosclerosis, most of the time the onset of a disease, like a heart attack or stroke, is brought on by sudden blockage of an artery. This abrupt closure is due to formation of a blood clot (thrombus) caused by the rupture of a small young plaque.3,4 In the heart the process is called “a coronary artery thrombosis” – a term interchangeable for “heart attack,” because essentially all heart attacks are due to the sudden formation of a thrombus.
These deadly lesions, referred to as “fatty plaques,” are soft and filled with white blood cells (pus cells) and necrotic (dead) materials. In your mind, you can accurately picture these volatile plaques as “sores” or “pustules lining the artery walls.” Fortunately, these young plaques are also the easiest and fastest component of the artery disease to heal (reverse). Therefore, within days, if not hours, of taking corrective actions (a healthy diet and judicious use of medications) you dramatically reduce your risk of a tragedy, like a heart attack or stroke.
The more mature part of this disease develops over many years. This established plaque is filled with scar tissue and calcium – and as a result, is very solid. This is where the name “hardening of the arteries” comes from. Therefore, reversing this established component comes very slowly with time and effort (if at all).
Any area of advanced artery disease (atherosclerosis) is made up of a spectrum of all stages of development from early, soft, fatty, to mature, hard, fibrous, plaques. Atherosclerosis is not like indestructible concrete. Instead, you should visualize this disease as an actively developing process in your arteries – there is ongoing injury taking place at the same time that the arteries are attempting to heal themselves. Unfortunately, the disease progresses because the forces of injury, mostly from the bad diet, far outpace the body’s ability to heal.
Your efforts to reverse this disease have the potential to reap phenomenal improvement in your symptoms (like chest pains, shortness of breath, and fatigue), almost overnight. Small changes in the size of the opening in the artery through which the blood flows will improve a patient’s symptoms far more than might be expected – because the volume of the flow of blood to the tissues increases greatly with even small increases in diameter of an artery.
Consider carefully the opportunity for rapid healing you have before you:
- First: small, but dangerous, young plaques, stabilize and reverse quickly;
- Second: a small increase in the diameter of an artery causes great improvements in flow.
Powerful Healing is Within Your Reach – Diet and Drugs Reverse Disease
Atherosclerosis is not sledge-hammer resistant rock. This is tissue that can heal under the proper conditions. You can create this healing environment cost-free with a change in diet (low-fat, whole plant foods) and habits (quit smoking). A small, but important, addition for the improvement in the conditions for healing can be accomplished with the use of cholesterol-lowering medications.
A study of 409 patients over an average time period of 5 years found intensive treatment with a very low-fat diet (10% fat), regular exercise and enough cholesterol-lowering medication to achieve an LDL “bad” cholesterol below 90 mg/dl resulted in great improvement in patients with severe heart disease compared to a group of patients who continued to be cared for poorly.5 Patients with coronary artery disease were divided into three groups based on the intensity of treatment they received. Those in the “maximum” treatment group had a 6.6% chance of suffering a heart artery related event* compared to 30.6% in those who had poor treatment (not on diet or drugs or who were smoking). Abnormalities of flow of blood through the coronary arteries to the heart muscle were measured with a heart scan (PET scan). Those in the maximum treatment group showed improvement in their circulation to the heart after 2.6 years, while those in the poor treatment group showed worsening of their circulation.
There was also an intermediate group called “moderate treatment.” They were on the American Heart Association Diet with 20% to 30% of the calories from fat and they were on cholesterol-lowering drugs. At the end of five years, 20.3% of these patients had cardiac events and after 2.6 years their scans showed worsening of their heart circulation. Thus, this approach, commonly prescribed by most practicing doctors, causes coronary artery disease to worsen, and more coronary events to occur.
The total cholesterol levels achieved by the three groups were an average of 140 mg/dl for the maximum treatment group, 184 mg/dl for the moderate group, and 226 for the poor group. The death rates from any cause were 3.3%, 15%, and 13%, respectively.
* Heart related events were cardiac deaths, heart attack, angioplasty, angiograms, bypass surgery, or stroke.
The Maximum Treatment You Deserve
There are many questions still to be answered about what is the ideal way to treat someone with artery disease. However, based upon what is presently known, this is the way I treat my patients with coronary artery disease. (The principles for the reversal of artery disease apply to all of the conditions of artery closure listed above, from hearing loss to impotence.):
1) I first determine if they have serious coronary artery disease – especially if they have been told they are candidates for heart surgery. This involves evaluation of their need for serious surgical interventions like an angiogram, angioplasty and/or bypass surgery. Don’t take this test lightly; an angiogram is a preoperative test. The actual need for invasive surgery (angioplasty, bypass) is determined by exploring the legitimate reason(s) for performing these procedures:
- First indication: Incapacitating Chest Pain. Does the patient have incapacitating chest pain unrelieved by good medical therapy (a low-fat diet and medications)? In general, incapacitating chest pain is the only indication for angioplasty, because this procedure has not been shown to save lives.
- Second indication: Lifesaving. Does the patient have a condition that is known to respond to surgery with the result of living longer? The only clear indication that bypass surgery has the potential to be lifesaving is finding a damaged left ventricle (heart chamber) so that the patient’s ejection fraction is now 50% or less (normal is 65%).6 This can be determined by a noninvasive echocardiogram. In this case bypass surgery (not angioplasty) has an 18% survival advantage over medical treatment after 10 years of follow-up.6 If the ejection fraction is above 50% then there is no survival advantage. (See the McDougall Program for a Healthy Heart for details.)
2) I place them on a low-fat, plant-based diet (the McDougall diet). This involves education that can be obtained from our books and website (free), but is most effectively accomplished at our 12-day online course. The study discussed above was far less strict than the diet I prescribe. Why am I so much more restrictive? I go for the “biggest medicine” I can find, because I’m looking for the best results possible for my patients. Besides, as you will discover, the diet I prescribe is actually the easiest one to follow for a lifetime.
3) I prescribe sufficient cholesterol-lowering medication to achieve a total cholesterol below 150 mg/dl (LDL below 90 mg/dl). I usually use statins and right now I prefer Pravachol. However, a cholesterol-binding agent like colestipol (Colestid) or cholestyramine (Questran) is as good a choice.
4) I prescribe one baby aspirin a day.
5) I prescribe moderate daily exercise – after the diet has been started. I begin with a recommendation to start with reasonable amounts and working up slowly. A patient should be able to carry on a normal conversation without becoming breathless while exercising.
6) I insist on weight loss. The diet and exercise program above will be sufficient for most people to achieve trim body weight. However, the few who cannot, I place on the Maximum Weight Loss Program, which limits their intake of flour products (breads, bagels and pastas), fruits, juices and other simple sugars. It encourages more rice, corn, potatoes, beans and green and yellow vegetables. Smaller more frequent meals are also encouraged; as is more exercise.
7) There may be some merit for the use of a beta blocker medication, like Metoprolol and/or an ACE inhibitor medication, like Zestril, after a heart attack.7 I’m not sure because the pharmaceutical companies have manipulated the research so much it is hard for a doctor to know what is true these days when it comes to drugs.
This is a very simple, low-tech, safe, almost cost-free, but highly effective way to clean out your arteries and the results usually happen faster than you would ever expect. However, all of these changes in diet and medication should be done under the supervision of a doctor experienced in this kind of care.
References:
1) Holman R. The natural history of atherosclerosis. The early aortic lesions as seen in New Orleans in the middle 20th century. Am J Pathol 1958;34:209.
2) Page IH. Prediction of coronary heart disease based on clinical suspicion, age, total cholesterol, and triglyceride. Circulation. 1970 Oct;42(4):625-45.
3) Kullo IJ. Vulnerable plaque: pathobiology and clinical implications. Ann Intern Med. 1998 Dec 15;129(12):1050-60.
4) Zhou J. Plaque pathology and coronary thrombosis in the pathogenesis of acute coronary syndromes. Scand J Clin Lab Invest Suppl. 1999;230:3-11.
5) Sdringola S. Combined intense lifestyle and pharmacologic lipid treatment further reduce coronary events and myocardial perfusion abnormalities compared with usual-care cholesterol-lowering drugs in coronary artery disease. J Am Coll Cardiol. 2003 Jan 15;41(2):263-72.
6) Alderman EL. Ten-year follow-up of survival and myocardial infarction in the randomized Coronary Artery Surgery Study. Circulation. 1990 Nov;82(5):1629-46.
7) Hostetter JC. Should everyone with a recent myocardial infarction receive a beta-blocker and an ACE inhibitor? Cleve Clin J Med. 2003 Jan;70(1):46-8.
Recommended Articles
Arsenic In Rice

Vitamin D: Values for Normal Are Exaggerated

Join the Conversation!
Have a question, a helpful tip, or a story from your journey? Add it below - your voice matters.