


Protein Overload

By John McDougall, MD
Muscle, vitality, strength, power, energy, vigor, aggressiveness, and liveliness are words that come to mind when people think of the benefits of protein in their diet. The truth is quite the opposite. Bone loss, osteoporisis, kidney damage, kidney stones, immune dysfunction, arthritis, cancer promotion, low-energy, and overall poor health are the real consequences from overemphasizing protein. Protein serves as raw material to build tissues. Without sufficient protein from your diet, your body would be in trouble – but, aside from starvation, this never happens. Yes, a little protein is good, but more is not better. Protein consumed beyond our needs is a health hazard as devastating as excess dietary fat and cholesterol. Unfortunately, almost everyone on the typical Western diet is overburdened with protein to the point of physical collapse. The public has almost no awareness of problems of protein overload, but scientists have known about the damaging effects of excess protein for more than a century.
In his book, Physiology Economy in Nutrition, Russell Henry Chittenden, former President of the American Physiological Society (APS) and Professor of Physiological Chemistry at Yale, wrote in 1905, “Proteid (protein) decomposition products are a constant menace to the well-being of the body; any quantity of proteid or albuminous food beyond the real requirements of the body may prove distinctly injurious…Further, it requires no imagination to understand the constant strain upon the liver and kidneys, to say nothing of the possible influence upon the central and peripheral parts of the nervous system, by these nitrogenous waste products which the body ordinarily gets rid of as speedily as possible.”1
A Cluttered House
Say you are building a house that requires one hundred sheets of plywood, but the lumberyard delivers two hundred sheets. Initially, you might think this is a good thing – a real windfall. But what do you really have? A big pile of expensive lumber cluttering your yard. The mess is an eyesore, a fire hazard, a potential source of physical injury and it detracts from your property value. Disposal of the excess lumber will be costly and could result in physical injury. To make matters worse, the lumberyard delivered “Fire Retardant Treated” (FRT) plywood. The fire-retardants used are very acidic and under humid conditions the acids weaken the lumber, leading to a potential structural failure of your house – a catastrophic threat to life and limb – not to mention your pocketbook.2
Lesson Learned: When building a house, take delivery of only the amount of lumber you actually need – and use only the safest construction materials.

What are Your Construction (Protein) Needs?
Protein from your diet is required to build new cells, synthesize hormones, and repair damaged and worn out tissues. So how much do you need?
The protein lost from the body each day from shedding skin, sloughing intestine, and other miscellaneous losses is about 3 grams per day (0.05 grams/Kg).3 Add to this loss other physiological requirements, such as growth and repairs. The final tally, based on solid scientific research, is: your total daily need for protein is about 20 to 30 grams.4,5 Plant proteins easily meet these needs.6
So what are people consuming? Those living in many rural Asian societies consume about 40 to 60 grams from their diet of starch (mostly rice) with vegetables.6 On the Western diet, typical food choices centered around meat and dairy products, “a well-balanced diet,” provides about 100 to 160 grams of protein a day. A traditional Eskimo, eating marine animals, or someone on the Atkins diet, from various kinds of meat and dairy, might be consuming 200 to 400 grams a day.7 Notice that there can be a 10-fold (1000%) difference from our basic requirements and the amount some people consume. The resilience of the human body allows for survival under conditions of incredible over-consumption.
Protein for the Human Body
| Situation | Protein*
(grams per day) |
Protein
(% of calories) |
| Daily Protein Loss | 3 grams | Less than 1% |
| Minimal Requirements | 20-30 grams | 4%-5% |
| Breast-fed Infant | 3-12 grams | 5%-6.3% |
| Asian Diet | 40-70 grams | 8%-14% |
| McDougall Diet | 35-75 grams | 7%-15% |
| Western Diet | 75-160 grams | 15%-32% |
| Zone Diet | 150 grams | 30% |
| South Beach Diet | 100-250 grams | 20%-70% |
| Atkins Diet | 150-359 grams | 30%70 |
*Calculations based on 2000 calories consumed for adults. Calories consumed on a weight loss program may often be less than 2000 a day. In this case, the absolute amount of protein would be proportionally less. Breast-fed infants consume about 350-1100 calories a day.
Once the body’s needs are met, then the excess must be removed. The liver converts the excess protein into urea and other nitrogen-containing breakdown products, which are finally eliminated through the kidneys as part of the urine.
The Fate of Excess Protein?
There are two possible fates for excess nutrients: They can be stored, like excess dietary fats and oils are stored in the body fat (adipose) tissue of our belly, thighs and buttocks – or the excesses can be eliminated. If protein were stored it would be deposited in our muscle tissues and people on the Western diet would all look like bodybuilders. Obviously, excess protein is not stored. Protein consumed in excess of the body’s needs therefore must be eliminated, with some effort and often at great expense to our health.
Excess Protein Burdens the Kidneys and Liver
Processing all that excess dietary protein – as much as 300 grams (10 ounces) a day –causes wear and tear on the kidneys; and as a result, on average, 25% of kidney function is lost over a lifetime (70 years) from consuming the Western diet.8,9 Fortunately, the kidneys are built with large reserve capacity and the effects of losing one-quarter of kidney function are of no consequence for otherwise healthy people. However, people who have already lost kidney function for other reasons – from an accident, donation of a kidney, infection, diabetes, and hypertension – may suffer life-threatening consequences from a diet no higher in protein than the average American consumes.10,11
The time-honored fundamental treatment for people with failing kidneys is a low-protein diet. End-stage kidney failure, requiring dialysis, can usually be postponed or avoided by patients fortunate enough to learn about the benefits of a low-protein diet.10-13
People suffering with liver failure are also placed on diets low in protein as fundamental therapy – short of a liver transplant, this is the most important therapy they will receive. During the end stages of liver failure, patients will often fall into a coma from the build-up of protein breakdown products (hepatic coma). A change to a cost-free, very low-protein diet can cause these dying people to awaken. Well planned, plant-food based diets are particularly effective with both kidney and liver disease.14,15
Excess Protein Damages the Bones = Osteoporosis
Worldwide, rates of hip fractures (and kidney stones) increase with increasing animal protein consumption (including dairy products). For example, people from the USA, Canada, Norway, Sweden, Australia, and New Zealand have the highest rates of osteoporosis.15,16 The lowest rates are among people who eat the fewest animal-derived foods (these people are also on lower calcium diets) – like the people from rural Asia and rural Africa.15,16
Osteoporosis is caused by several controllable factors; however, the most important one is the foods we choose – especially the amount of animal protein and the foods high in acid.17-19 The high acid foods are meat, poultry, fish, seafood, and hard cheeses – parmesan cheese is the most acidic of all foods commonly consumed.20 This acid must be neutralized by the body.21 Carbonate, citrate and sodium are alkaline materials released from the bones to neutralize the acids. Fruits and vegetables are alkaline and as a result a diet high in these plant foods will neutralize acid and preserve bones. The acidic condition of the body caused by the Western diet also raises cortisol (steroid) levels. 22 Elevated cortisol causes severe chronic bone loss – just like giving steroid medication for arthritis causes severe osteoporosis.
Compare the acid load of various foods:
(Renal Acid Load per 100 calories)23,24
| Beef | 6.3 |
| Chicken | 7.0 |
| Fish (Cod) | 9.3 |
| Cheddar Cheese | 10.0 |
| Potato | -5.0 |
| Peas | 1.0 |
| Wheat Flour | 1.0 |
| Banana | -6.0 |
| Apples | -5.0 |
| Spinach | -56.0 |
| Tomatoes | -18 |
(A positive value indicates acidic, whereas a negative value indicates alkaline.)
Consequence Two: Kidney Stones
Once materials are released from the solid bone, the calcium and other bone substances move through the blood stream to the kidneys where they are eliminated in the urine. In an effort to remove the overabundance of waste protein, the flow of blood through the kidneys (glomerular filtration rate) increases – the result: calcium is filtered out of the body. Naturally, the kidneys attempt to return much of this filtered calcium back to the body; unfortunately, the acid and sulfur-containing amino acids from the animal foods thwart the body’s attempts to conserve calcium. The final result is each 10 grams of dietary protein in excess of our needs (30 grams daily) increases daily urinary calcium loss by 16 mg. Another way of looking at the effects is: doubling protein intake from our diet increases the loss of calcium in our urine by 50%.25 Plant proteins (plant food-bases) do not have these calcium and bone losing effects under normal living conditions.
Once this bone material arrives in the collecting systems of the kidney it easily precipitates into sold formations known as kidney stones.27 Over 90% of kidney stones found in people following a high-protein, Western diet are formed primarily of bone-derived calcium. Following a healthy diet is the best way to prevent kidney stones.28
Toxic Sulfur Distinguishes Animal Foods
The qualities of the proteins we consume are as important as the quantities. One very important distinction between animal and plant-derived protein is that animal proteins contain very large amounts of the basic element sulfur. This sulfur is found as two of the twenty primary amino acids, methionine and cysteine. Derived from these two primary sulfur-containing amino acids are several other sulfur-containing amino acids – these are keto-methionine, cystine, homocysteine, cystathionine, taurine, cysteic acid.
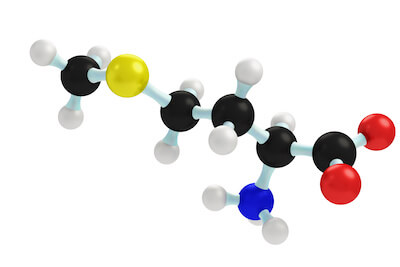
The yellow sphere represents the element sulfur.
Compare the relative amounts of the sulfur containing amino acid, methionine, found in these common foods (based on the same number of calories):24
- Beef provides 4 times more than pinto beans
- Eggs have 4 times more than corn
- Cheddar cheese has 5 times more than white potatoes
- Chicken provides 7 times more than rice
- Tuna provides 12 times more than sweet potatoes
Even though sulfur-containing amino acids are essential for our survival, an excess of these amino acids beyond our needs places a critical burden upon our body and detracts from our health in six important ways:
1) Amino acids, as the name implies are acids; the sulfur-containing amino acids are the strongest acids of all, they breakdown into powerful sulfuric acid. Excess acid, as discussed above, is a primary cause of bone loss leading to osteoporosis and kidney stone formation.29
2) Methionine is metabolized into homocysteine – animal foods are the major source of the amino acid, homocysteine, in people – the more meat in the diet, the higher a person’s blood level of homocysteine. A diet high in fruits and vegetables lowers the levels of this amino acid. Epidemiological and clinical studies have proven homocysteine to be an independent risk factor for heart attacks, strokes, closure of the arteries to the legs (peripheral vascular disease), blood clots in the legs (venous thrombosis), thinking problems (cognitive impairment), and even worse mental troubles, like dementia, Alzheimer’s disease, and depression.30
3) Sulfur feeds cancerous tumors Cancer cell metabolism is dependent upon methionine being in the diet; whereas, normal cells can grow on a methionine-free diet (feeding off of other sulfur-containing amino acids). This methionine-dependency has been demonstrated for breast, lung, colon, kidney, melanoma, and brain cancers.31,32 Increasing methionine in the diet of animals promotes the growth of cancer.33
There is also evidence of cancer promoting effects of methionine mediated through a powerful growth stimulating hormone, called insulin-like growth factor – 1 (IGF-1).34 Meat and dairy products raise IGF-1 levels and promote the growth of cancers of the breast, colon, prostate, and lung.35
4) Sulfur from sulfur-containing amino acids is known to be toxic to the tissues of the intestine, and to have deleterious effects on the human colon, even at low levels.36 The consequence of a diet of high-methionine (animal) foods may be a life-threatening inflammatory bowel disease, called ulcerative colitis.37-38
5) Sulfur restriction prolongs life.39 Almost seventy years ago, restricting food consumption was found to prolong the life of animals by changing the fundamental rate at which aging occurs.40 Restriction of methionine in the diet has also been shown to prolong the life of experimental animals. By no coincidence, a diet based on plant foods is inherently low in both calories and methionine – thus the easiest and most effective means to a long and healthy life.
6) Possibly a stronger motivation to keep protein, and especially methionine-rich animal protein, out of your diet is foul smelling odors – halitosis, body odor, and noxious flatus – akin to the smell of rotten eggs – are direct results of the sulfur (animal protein) you eat.41,42
Do Not Waste Your Health Away
Animal foods, full of protein waste, promote poor health and early death by accelerating the aging process and increasing the risk of diseases, like heart disease, diabetes, and cancer, that in their own right, cause premature death. From now on, think of the excess protein you consume as garbage that must be disposed of in order to avoid toxic waste accumulation. Obviously, the best action is to avoid the excess in the first place and this is most easily accomplished by choosing a diet based on starches, vegetables, and fruits. Within a few days of changing to a healthy diet, most of the waste will be gone and the damaged tissues will begin healing.
Unfortunately, you will find little support for such an obvious, inexpensive, and scientifically-supported approach – especially when the common masses of people worldwide are ignorant of the truth – most are gobbling down as much protein as they can stuff in their mouths – and the food industry is supporting this behavior by advertising their products as “high-protein” and “Atkins-approved” – as if this was somehow good for the body. This paradox is age-old, and because it is ruled by emotions, rather than clear thinking, a change in mind-set in your lifetime, should not be expected.
Two thousand years ago, in this Bible passage, Paul asked for tolerance between meat eaters and vegetarians (Romans 14:1-2). “One man’s faith allows him to eat everything, but another man whose faith is weak, eats only vegetables. The man who eats everything must not look down on him who does not, and the man who does not eat everything must not condemn the man who does…” Do not wait for a consensus before you take action.
References:
1) Chittenden, R. H. (1905). Physiological economy in nutrition, with special reference to the minimal protein requirement of the healthy man. An experimental study. New York: Frederick A. Stokes Company.
2) Fire Retardant Treated Plywood: http://www.nexsenpruet.com/library/docs/NPCOL1_624753_1.pdf
3) Calloway DH. Sweat and miscellaneous nitrogen losses in human balance studies.
J Nutr. 1971 Jun;101(6):775-86.
4) Hegsted DM.. Minimum protein requirements of adults. Am J Clin Nutr. 1968 May; 21(5): 352-7.
5) Dole V. Dietary treatment of hypertension: clinical and metabolic studies of patients on the rice-fruit diet, J Clin Invest, 1950; 29: 1189-1206.
6) Millward DJ. The nutritional value of plant-based diets in relation to human amino acid and protein requirements. Proc Nutr Soc. 1999 May;58(2):249-60.
7) Mazess RB. Bone mineral content of North Alaskan Eskimos. Am J Clin Nutr. 1974 Sep; 27(9): 916-25.
8) Brenner BM. Dietary protein intake and the progressive nature of kidney disease: the role of hemodynamically mediated glomerular injury in the pathogenesis of progressive glomerular sclerosis in aging, renal ablation, and intrinsic renal disease. N Engl J Med. 1982 Sep 9; 307(11): 652-9.
9) Meyer TW. Dietary protein intake and progressive glomerular sclerosis: the role of capillary hypertension and hyperperfusion in the progression of renal disease. Ann Intern Med. 1983 May; 98(5 Pt 2): 832-8.
10) Hansen HP. Effect of dietary protein restriction on prognosis in patients with diabetic nephropathy. Kidney Int. 2002 Jul; 62(1): 220-8.
11) Biesenbach G. Effect of mild dietary protein restriction on urinary protein excretion in patients with renal transplant fibrosis. Wien Med Wochenschr. 1996; 146(4): 75-8.
12) Pedrini MT. The effect of dietary protein restriction on the progression of diabetic and nondiabetic renal diseases: a meta-analysis. Ann Intern Med. 1996 Apr 1;124(7):627-32.
13) Cupisti A. Vegetarian diet alternated with conventional low-protein diet for patients with chronic renal failure. J Ren Nutr. 2002 Jan;12(1):32-7.
14) Bianchi GP. Vegetable versus animal protein diet in cirrhotic patients with chronic encephalopathy. A randomized cross-over comparison. J Intern Med. 1993 May; 233(5): 385-92.
15) Abelow B. Cross-cultural association between dietary animal protein and hip fracture: a hypothesis. Calcific Tissue Int 50:14-8, 1992.
16) Frassetto LA . Worldwide incidence of hip fracture in elderly women: relation to consumption of animal and vegetable foods. J Gerontol A Biol Sci Med Sci. 2000 Oct;55(10):M585-92.
17) Maurer M. Neutralization of Western diet inhibits bone resorption independently of K intake and reduces cortisol secretion in humans. Am J Physiol Renal Physiol. 2003 Jan;284(1):F32-40.
18) Remer T. Influence of diet on acid-base balance. Semin Dial. 2000 Jul-Aug;13(4):221-6.
19) Frassetto L. Diet, evolution and aging–the pathophysiologic effects of the post-agricultural inversion of the potassium-to-sodium and base-to-chloride ratios in the human diet. Eur J Nutr. 2001 Oct;40(5):200-13.
20) Remer T. Potential renal acid load of foods and its influence on urine pH. J Am Diet Assoc. 1995 Jul;95(7):791-7.
21) Barzel US. Excess dietary protein can adversely affect bone. J Nutr. 1998 Jun;128(6):1051-3.
22) Maurer M. Neutralization of Western diet inhibits bone resorption independently of K intake and reduces cortisol secretion in humans. Am J Physiol Renal Physiol. 2003 Jan; 284(1): F32-40. Epub 2002 Sep 24.
23) Remer T. Potential renal acid load of foods and its influence on urine pH. J Am Diet Assoc. 1995 Jul;95(7):791-7.
24) J Pennington. Bowes & Church’s Food Values of Portions Commonly Used. 17th Ed. Lippincott. Philadelphia- New York. 1998.
25) Massey LK . Dietary animal and plant protein and human bone health: a whole foods approach. J Nutr. 2003 Mar; 133(3): 862S-865S.
26) Jenkins DJ. Effect of high vegetable protein diets on urinary calcium loss in middle-aged men and women. Eur J Clin Nutr. 2003 Feb;57(2):376-82.
27) Lemann J Jr. Relationship between urinary calcium and net acid excretion as determined by dietary protein and potassium: a review. Nephron. 1999; 81 Suppl 1: 18-25.
28) Delvecchio FC. Medical management of stone disease. Curr Opin Urol. 2003 May; 13(3): 229-33.
29) Remer T. Influence of diet on acid-base balance. Semin Dial. 2000 Jul-Aug; 13(4): 221-6.
30) Troen AM. The atherogenic effect of excess methionine intake. Proc Natl Acad Sci U S A. 2003 Dec 9; 100(25): 15089-94.
31) Cellarier E. Methionine dependency and cancer treatment. Cancer Treat Rev. 2003 Dec; 29(6): 489-99.
32) Epner DE. Nutrient intake and nutritional indexes in adults with metastatic cancer on a phase I clinical trial of dietary methionine restriction. Nutr Cancer. 2002; 42(2): 158-66.
33) Paulsen JE. Growth stimulation of intestinal tumours in Apc(Min/+) mice by dietary L-methionine supplementation. Anticancer Res. 2001 Sep-Oct; 21(5): 3281-4.
34) Stubbs AK. Nutrient-hormone interaction in the ovine liver: methionine supply selectively modulates growth hormone-induced IGF-I gene expression. J Endocrinol. 2002 Aug; 174(2): 335-41.
35) Yu H. Role of the insulin-like growth factor family in cancer development and progression. J Natl Cancer Inst. 2000 Sep 20;92(18):1472-89.
36) Levine J. Fecal hydrogen sulfide production in ulcerative colitis. Am J Gastroenterol. 1998 Jan;93(1):83-7.
37) Roediger W. Sulphide impairment of substrate oxidation in rat colonocytes: a biochemical basis for ulcerative colitis? Clin Sci (Lond). 1993 Nov;85(5):623-7.
38) Christl S. Effect of sodium sulfide on cell proliferation of colonic mucosa. Gastroenterology 1994; 106:A664 (abstr).
39) Zimmerman JA. Nutritional control of aging. Exp Gerontol. 2003 Jan-Feb; 38(1-2): 47-52.
40) McCay C. The effect of retarded growth upon length of lifespan and upon ultimate body size. J Nutr. 1935; 10: 63-79.
41) McDougall J. Halitosis Is More than Bad Breath . McDougall Newsletter. January 2002 at www.drmcdougall.com.
42) McDougall J. Bad Farts? Meat Stinks! McDougall Newsletter. August 2002 at www.drmcdougall.com.
Recommended Articles
The Latest Scams from the Diabetic Industry

When Friends Ask: Why Do You Avoid Adding Vegetable Oils?
Join the Conversation!
Have a question, a helpful tip, or a story from your journey? Add it below - your voice matters.