


My Stomach’s on Fire and I Can’t Put it Out
This article originally appeared in the February 2002 McDougall Newsletter.
By John McDougall, MD
Most of us call this common complaint indigestion, but doctors call it dyspepsia. Indigestion is an old English word that means, “lack of adequate digestion.” Dyspepsia means impaired gastric or digestive function. But what we are trying to communicate is “suffering from discomfort, burning, or pain in our upper central abdominal area.” We explain our feelings by saying we have an upset stomach, heartburn, acid indigestion, and acid regurgitation.
Fifty-six per cent of the people in Western countries report they have suffered from heartburn at some time in the past and 36% have symptoms at least once every 4-6 months.1 Half to two-thirds of pregnant women suffer heartburn during pregnancy. Patients with indigestion and acid reflux report worse emotional well-being than do people with heart failure, symptomatic heart disease, diabetes and hypertension.2,3
My guess, based on people I have seen, is that this problem is even more common than reported. Walk down the medication aisles of your local supermarket or drug store and you’ll see shelves of liquids and tablets intended to neutralize the acid, and pills to prevent acid production. Most people rely on self-medication to treat their discomfort, but the prescription side of this heartburn business is huge. The first and third largest sum of money spent on any prescription medication in the year 2000 was for two antacids, Prilosec and Prevacid.4 This amounted to nearly $7 billion spent in the United States for that year – just for just two medications.
GERD is the (Key) Word
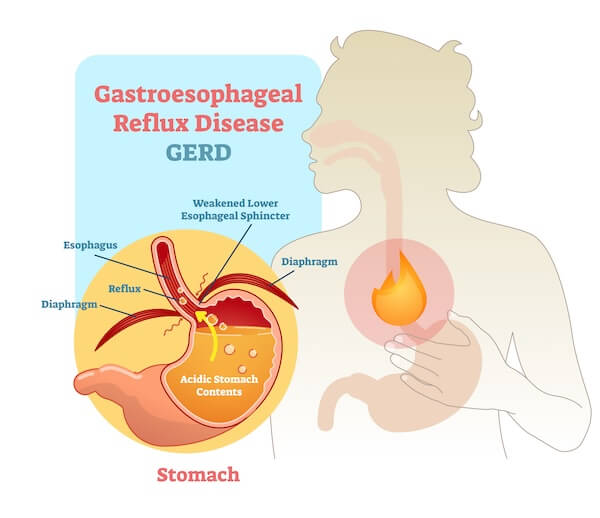
The source of almost half the indigestion suffered is from the retrograde flow of the stomach contents up into the esophagus – a condition called gastro-esophageal reflux disease or GERD. This condition is often felt as a burning feeling behind the sternum (breastbone) that radiates up toward the throat and is worsened by a meal or by lying down. The primary cause of the symptoms and associated tissue injury is the presence of stomach acid and other digestive juices outside of the stomach. GERD occurs in 7% of people daily and 36% of people at least once a month.5 The diagnosis is usually made by the doctor listening to the patient’s symptoms. Further evaluation of the disease is most commonly done by looking at the esophagus through a tube known as an endoscope. However, no evidence of disease is found by this examination in a high percentage of people with symptoms of GERD.
Acid Can Burn Your Mouth, Throat and Lungs
Complications from acid reflux, GERD, can be as minor as heartburn or as severe as deep ulcers and cancer. When the acid refluxes into the mouth and is inhaled into the lungs, serious disease, like erosion of the teeth and asthma, can result.
Erosion of the Teeth
Erosion of the enamel of the teeth is caused by the reflux of stomach acid contents into the mouth. The acid destroys the tooth enamel and the loss is permanent. This condition is commonly seen with a weight control method known as bulimia, which is used by 4% to 10% of college age women. Dental erosion is seen in 69% of patients with bulimia, due to acid on the teeth from repeated vomiting. When people without bulimia, but with dental erosions, were studied it was found that 83% had evidence of GERD.6 This relationship was confirmed when 40% to 70% of people with GERD were found to have erosions.6 The worse the reflux the more likely the finding of erosions.
Damage to the oral-sinus cavities from GERD:
Dental Erosions
Mouth Ulcers
Loss of taste
Mouth pain
Sinusitis
Ear pain and inflammation
Asthma and Upper Airway Problems
Acid refluxed up into the back of the throat can be inhaled into the bronchial (airway) tubes and burn them, causing constriction, swelling, and large amounts of mucus production. Somewhere between 34% and 89% of asthmatics have GERD.7 Seventy-five percent of children with asthma have GERD.7 Patients with asthma caused by GERD commonly complain of heartburn, regurgitation, and difficulty swallowing. Their asthma is worsened by meals and when lying down, or sleeping. Treatment with a healthy diet that reduces the chances of reflux, raising the head of the bed by four to six inches, and as a last resort, antacids, will relieve asthma and many other breathing problems, and reduce the need for asthma medications.8
Airway problems from GERD:
Asthma
Chronic cough
Bronchitis
Emphysema
Pneumonia
Laryngitis
Chronic Hoarseness
Inflammation of throat
Vocal cord ulcers
Noncardiac chest pain
The Causes of Indigestion and GERD
Gastroesophageal reflux disease (GERD) occurs when the stomach acid contacts the tissues of the esophagus, mouth, sinuses, and lungs. For this to occur, acid must reflux past the “natural anti-reflux barrier” between the esophagus and the stomach. At rest, the most important component of this barrier is the lower esophageal sphincter (LES). The LES is an area of increased muscular activity, which produces pressures which keep the opening between the esophagus and stomach closed most of the time when we are not swallowing. However, when this LES relaxes at inappropriate times, acid can reflux out of the stomach causing GERD. There are two general reasons the LES functions poorly. The first is due to actual structural damage of the LES caused by years of an unhealthy diet with resulting constipation and failing to squat when defecating. Second, many of the foods and beverages we consume cause this sphincter to transiently relax permitting the reflux of acid.
A Low Fiber Diet Permanently Damages the Anti-reflux Barrier
At least one well respected researcher of gastrointestinal diseases believes that more than 90 percent of the GERD found among people living in the Western world is a direct result of constipation.9 Physical efforts to evacuate a hard, constipated stool out of the rectum into the toilet cause severe straining that pushes the stomach from its normal position in the abdominal cavity, up into the chest. (For a moment, picture a red-faced person sitting on the toilet seat grunting and groaning in an effort to pass his tiny rock-hard stool). As a result of all that physical effort, the natural opening in the muscular diaphragm through which the esophagus passes is widened, creating a hiatal hernia. Eventually, part of the stomach lies in the chest cavity, then with each breath negative pressures are created that pull acid up into the esophagus. The strength of the LES is also gradually weakened over time as a result of chronic straining to defecate.
Constipation is caused by a diet low in dietary fiber and by dairy products.10,11 Dietary fiber is only present in plant foods – naturally, the meat and dairy-based, highly refined American diet is very low in fiber and constipating. The American diet contains about six to ten grams of fiber daily, whereas a healthy diet based on starches, vegetables and fruits has 40 to 100 grams of dietary fiber. Dairy products can paralyze bowel activity resulting in constipation, and the protein is the cause – so low-fat dairy will be at least as harmful.
Another source of damage to the LES and a cause of hiatal hernia is from abandoning the historically common and worldwide practice of squatting to defecate.9 Less force is required to evacuate the stool when in a squatted position over a hole in the ground rather than when on a high-seated toilet.
Another chronic dietary disease associated with indigestion and GERD is obesity.12 This association most likely reflects poor health, the presence of a hiatal hernia, and damage to the LES than any direct effect of extra body fat pushing on the stomach. However, excess body fat pushing on the stomach and tight clothing have been suspected of increasing acid reflux.
Short-Term Dietary Causes of (Transient) LES Dysfunction
Fat, chocolate, peppermint, onions, coffee, decaffeinated coffee and overdistention of the stomach are all believed to cause heartburn by decreasing the pressure of the lower esophageal sphincter and increasing the number of relaxations of this sphincter.14-27
Fat:
Thirty years ago a high-fat diet was recognized as a cause of acidity, heartburn and belching, and one doctor reported that a diet with no added fat cured 425 of 532 patients found to be fat-intolerant over a three year period of observation.13 Recent studies at the University of Virginia Health Sciences Center confirmed that fat causes heartburn.14 In 12 healthy volunteers and 11 patients with reflux esophagitis, saline or fat was infused into the duodenum (the first part of the small intestine). Fat directly aggravated reflux by increasing the number of LES relaxations. Other research has found the reflux of acid becomes progressively worse over the next three hours after eating a meal high in fat.15
Over-Eating:
The same group of researchers from the University of Virginia Health Sciences Center found that over-distention of the stomach caused indigestion.16 By inflating balloons which had been inserted in peoples’ stomachs the researchers produced an increase in the rate of LES relaxations. Their overall conclusion was that large fatty meals which distend the stomach are a major cause of heartburn. The pains were found to be even more frequent in people who drank a lot of coffee after meals and with smokers.
Onions, chocolate, and mints:
Onions, chocolate, and mints have all been shown to cause indigestion by relaxing the LES.17-21 The effects of onion on acid reflux and reflux symptoms were investigated in 16 normal subjects and 16 heartburn subjects.17 Subjects were studied by testing the acid in their esophagus two hours after the ingestion of a plain hamburger and a glass of ice water. The identical meal, with the addition of a slice of onion, was ingested on another day. Onions significantly increased all measures of heartburn in subjects and were found to be a potent and long-lasting cause of reflux in heartburn patients. Cooking onions destroys substances that are the cause of indigestion. This is why most people have no problems with cooked onions.
Chocolate syrup (even low-fat syrup) produces immediate and sustained decreases in LES pressure and symptomatic reflux in people.19 Approximately 40% of people surveyed had symptoms of heartburn after chocolate.5 However, in the same survey 76% of people said fatty foods caused their symptoms. Dark chocolate with its high fat content (50% fat), may therefore cause an even greater fall in LES pressure and more heartburn than low-fat chocolate.
Regular and Decaffeinated Coffee:
Coffee is upsetting to the stomach because it causes relaxation of the LES. Decaffeinated coffee also causes indigestion by reducing the LES function, but the effects are somewhat less.22-24 Caffeine, however, does not cause LES dysfunction. Another interesting finding is that regular ground coffee and decaffeinated coffee stimulate acid secretion by similar amounts. 25 This means substances in the coffee other than caffeine are causing the heartburn and reflux. More recent studies suggest that LES dysfunction and gastroesophageal reflux, rather than acid production, are responsible for the heartburn caused by coffee.26 Therefore, for relief, coffee drinkers must switch beverages to something like herbal tea or water, rather than “decaf.”
Even though there is considerably more indigestion among coffee drinkers, there is no increase in the risk of stomach or duodenal ulcers.27
Smoking Cigarettes and Alcohol:
Cigarette smoking and alcohol will lower LES and cause indigestion.28-30 However, most of the distress from alcoholic beverages comes from irritation of the stomach linings and the production of acids. Next month we will discuss important ways some alcoholic beverages, like wine and beer, cause stomach distress.
Citrus Fruits, Spices, and Tomatoes Are Irritating
Think about your reaction to drinking grapefruit juice or orange juice. Immediately my thoughts are of a sour stomach and burning indigestion. Citrus fruits, tomatoes, and spicy foods cause most of their distress by a direct irritating effect on the tissues of the esophagus and stomach, since they do not appear to lower LES pressure.31 Acidity is thought not to be the cause of the heartburn since neutralized orange juice also produces heartburn.21 The heartburn effects of fruit juice must result from the disruption of the fibers and other protective substances in the fruit caused when making the juice, because the whole fruit rarely causes distress in people.
I have also found raw vegetables more irritating than cooked. Some of the most troublesome are onions, green peppers, cucumbers and radishes.
Three meals chosen specifically to cause heartburn:
Investigators looking into the causes of heartburn have tried to find the meals that will reliably produce severe distress.32 They chose the following meals:
1) A McDonald’s Quarter Pounder, a small order of fries, and an 8-ounce chocolate milk shake.
2) A McDonald’s Sausage Biscuit with egg, one slice of cheese, 30 grams of raw onion and 8 ounces of Borden’s Dutch Chocolate Milk.
3) An 8-ounce Wendy’s Chili and 8 ounces of red wine.
The chili meal with wine produced the greatest numbers of reflux and the most severe heartburn for the first hour after the meal. The sausage biscuit meal, which had the highest fat content, produced the most severe heartburn 90 minutes after the meal. Of all three meals, the sausage biscuit meal produced the maximum heartburn, heartburn-related symptoms and acid reflux.33 And you wonder why prescription antacids are a $7 billion business in the US?
Some Common Medications That Relax the LES34
Calcium channel blockers (blood pressure pills)
Meperidine (Demerol)
Morphine
Dopamine
Beta-adrenergic antagonists
Diazepam (Valium)
Barbiturates
Theophylline (for asthma)
Progesterone
Medications for Treating GERD
There are several classes of medications which will offer some relief from GERD and indigestion.29 Liquid and tablet antacids, H2 receptor antagonists (see below), and proton pump inhibitors (see below) all reduce the amount of acid in the stomach. Some agents increase the LES pressure, like bethanecol (Edronax). Alginic acid (Protacid) forms a protective foam barrier and sucralfate (Carafate) buffers some of the acid. H2 receptor antagonists may cause mental changes, increased estrogen activity which can cause enlarged breasts in men, and changes in the metabolism of other medications.22 There is some concern that H2 receptor antagonists and proton pump inhibitors may cause stomach cancer with long-term use.34-35 Use any of these medications only as a last resort after you have tried the simple and safe actions listed at the end of this article.
Examples:
Liquid and Wafer Antacids:
Tums
Rolaids
Mylanta
Maalox
H2 receptor antagonists:
Cimetidine (Tagamet)
Ranitidine (Zantac)
Famotidine (Pepcid)
Nizatidine (Axid)
Proton pump inhibitors:
Lansoprazole (Prevacid)
Omeprazole (Prilosec)
Putting Out The Flames Forever
Most of my patients throw away their antacids on the first day of my program at St. Helena Hospital and never have to use them again unless they eat foods that are known to bother them. I also see almost overnight improvement in asthma, hoarseness, chronic cough, and sinusitis. They follow a diet based on starches with the addition of fruits and vegetables. Most of the food is cooked. In the beginning, their stomach and esophagus may be so raw from years of over-acidity and acid reflux that even water causes pain — they have to allow a few days for the inflammation to quiet down. In the interim period they sometimes benefit from antacids in the form of liquids or tablets to neutralize the acid, or pills to stop the production of acid. Raising the head of the bed by four to six inches by placing bricks or wood blocks under the head posts is of great help for those with the most reflux. In those very sensitive cases, extra care must be taken to eat small meals of plain, well-cooked, starches, vegetables and fruits. Spices should be avoided; however, sugar and salt are well-tolerated. Water should be the initial beverage in those with the most severe symptoms.
Even though considerable damage may have already occurred, to the point of causing LES dysfunction and a hiatal hernia, almost every patient can find relief with these simple steps, low in cost and free of side effects:
Ten Actions To Take To Quench the Fire
- Consume a plant-based diet, low in fat and high in fiber
- Avoid foods which aggravate the indigestion, such as raw onions, green peppers, cucumbers, radishes, and fruit juices, and hot spices
- Eat small meals frequently – Do not over-distend your stomach
- Lose weight if you are obese, and wear loose clothing
- Give up regular and decaffeinated coffee
- Whenever possible avoid medications which lower LES
- Raise the head of the bed four to six inches (extra pillows will not help – they only bend you at the middle)
- Avoid lying down within three hours of eating
- Stop cigarettes and alcohol
- Take antacid medications as a last resort.
References:
1. Bolin TD. Heartburn: community perceptions. J Gastroenterol Hepatol. 2000 Jan;15(1):35-9.
2. Revicki DA. The impact of gastroesophageal reflux disease on health-related quality of life. Am J Med. 1998 Mar;104(3):252-8.
3. Glise H. Quality of Life assessments in the evaluation of gastroesophageal reflux and peptic ulcer disease before, during and after treatment. Scand J Gastroenterol Suppl. 1995;208:133-5.
4. Prescription drug expenditures in the year 2000. Upward trend continue. A research report by The National Institute for Health Care Management. http://www.nihcm.org/.
5. Nebel O. Symptomatic gastroesophageal reflux: incidence and precipitating factors Am J Dig Dis21:953-6, 1976.
6. Schroeder P. Dental erosion and acid reflux disease. Ann Intrn Med 122:809-15, 1995.
7. Simpson W. Gastroesophageal reflux disease and asthma. Diagnosis and management. Arch Intrn Med 155: 798-803, 1995.
8. Hogan W. Medical treatment of supraesophageal complications of gastroesophageal reflux disease. Am J Med. 2001 Dec 3;111 Suppl 8A:197S-201S.
9. Sontag SJ Defining GERD. Yale J Biol Med. 1999 Mar-Jun;72 (2-3):69-80.
10. Scheppach W. Beneficial health effects of low-digestible carbohydrate consumption. Br J Nutr. 2001 Mar;85 Suppl 1:S23-30.
11. Iacono G. Intolerance of cow’s milk and chronic constipation in children. N Engl J Med. 1998 Oct 15;339(16):1100-4.
12. Woodward M. The prevalence of dyspepsia and use of antisecretory medication in North Glasgow: role of Helicobacter pylori vs. lifestyle factors. Aliment Pharmacol Ther. 1999 Nov;13(11):1505-9.
13. Childs, P. Dietary fat, dyspepsia, diarrhoea, and diabetes. Br J Surg 59:669-95, 1972.
14. Holloway RH Effect of intraduodenal fat on lower oesophageal sphincter function and gastro-oesophageal reflux.Gut. 1997 Apr;40(4):449-53.
15. Becker D. A comparison of high and low fat meals on postprandial esophageal acid exposure. Am J Gastroenterol. 1989 Jul;84(7):782-6.
16. Holloway RH. Gastric distention: a mechanism for postprandial gastroesophageal reflux. Gastroenterology. 1985 Oct;89(4):779-84.
17. Allen ML The effect of raw onions on acid reflux and reflux symptoms.
Am J Gastroenterol. 1990 Apr;85(4):377-80.
18. Murphy D. Chocolate and heartburn: evidence of increased esophageal acid exposure after chocolate ingestion. Am J Gastroenterol. 1988 Jun;83(6):633-6.
19. Babka J. On the genesis of heartburn. The effects of specific foods on the lower esophageal sphincter. Am J Dig Dis. 1973 May;18(5):391-7.
- Szarka L. Practical pointers for grappling with GERD. Heartburn gnaws at quality of life for many patients. Postgrad Med. 1999 Jun;105(7):88-90, 95-8, 103-6.
- Price S. Food sensitivity in reflux esophagitis. Am J Gastroenterol 75: 240-243, 1978.
- Van Deventer G. Lower esophageal sphincter pressure, acid secretion, and blood gastrin after coffee consumption. Dig Dis Sci. 1992 Apr;37(4):558-69.
- Wendl B. Effect of decaffeination of coffee or tea on gastro-oesophageal reflux. Aliment Pharmacol Ther 1994 Jun;8(3):283-7.
- Pehl C. The effect of decaffeination of coffee on gastro-oesophageal reflux in patients with reflux disease. Aliment Pharmacol Ther. 1997 Jun;11(3):483-6.
- Cohen S. Gastric acid secretion and lower-esophageal-sphincter pressure in response to coffee and caffeine. N Engl J Med. 1975 Oct 30;293(18):897-9.
- Cohen S. Pathogenesis of coffee-induced gastrointestinal symptoms.
N Engl J Med. 1980 Jul 17;303(3):122-4. - Elta GH Comparison of coffee intake and coffee-induced symptoms in patients with duodenal ulcer, nonulcer dyspepsia, and normal controls. Am J Gastroenterol. 1990 Oct;85(10):1339-42.
- Smit CF. Effect of cigarette smoking on gastropharyngeal and gastroesophageal reflux. Ann Otol Rhinol Laryngol. 2001 Feb;110(2):190-3.
- Weinberg D. The diagnosis and management of gastroesophageal reflux disease. Med Clin North Am. 1996 Mar;80(2):411-29.a
- Hogan W. Ethanol-induced acute esophageal motor dysfunction. J Appl Physiol. 1972 Jun;32(6):755-60.
- Cranley JP. Abnormal lower esophageal sphincter pressure responses in patients with orange juice-induced heartburn. Am J Gastroenterol. 1986 Feb;81(2):104-6.
- Rodriguez S. Meal type affects heartburn severity. Dig Dis Sci. 1998 Mar;43(3):485-90.
- Rodriguez S. The effects of capsaicin on reflux, gastric emptying and dyspepsia. Aliment Pharmacol Ther. 2000 Jan;14(1):129-34.
- Farrow DC. Gastroesophageal reflux disease, use of H2 receptor antagonists, and risk of esophageal and gastric cancer. Cancer Causes Control. 2000 Mar;11(3):231-8.
- Weinstein WM. Proton pump inhibitors and H. pylori infection: why the concern? Curr Gastroenterol Rep. 1999 Dec;1(6):507-10.
Recommended Articles

Mary's Mini-McDougall Diet® - An Overview

Can Exercise Lower Cholesterol?

Join the Conversation!
Have a question, a helpful tip, or a story from your journey? Add it below - your voice matters.